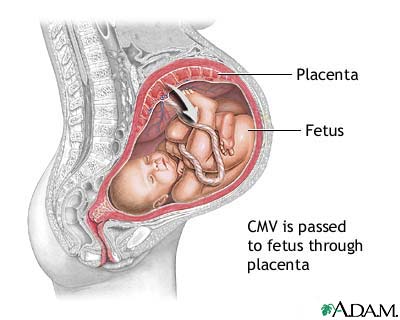
Concerns with Pregnancy & Cytomegalovirus (Mononucleosis):
- Cytomegalovirus (CMV) is the most common cause of congenital infection and complicates approximately 1% of all live births leading to permanent disabilities such as hearing loss, vision loss and cognitive impairment.
- CMV is most frequently identified as a viral cause of mental retardation and the leading non genetic cause of neurosensory hearing loss.
- Women who develop CMV infection in the first trimester are more likely to deliver fetuses with sensorineural hearing loss or mental retardation and cerebral palsy.
- In cases where maternal CMV infection is suspected, it is important to evaluate the risk to the fetus of being infected and/or symptomatically affected by CMV to provide appropriate counseling and guidance to parents.


Case Study:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3046747/
A healthy 29-year-old woman with a well-dated spontaneous conception was seen for routine ultrasound examination at 18-0/7 weeks of gestation. The fetus was noted to have echogenic bowel and intrauterine growth restriction (IUGR) with an estimated fetal weight in the 9th percentile. Her past obstetric history was remarkable for severe preeclampsia resulting in an induction of labor and vaginal delivery at 34 weeks of gestation 2 years earlier.
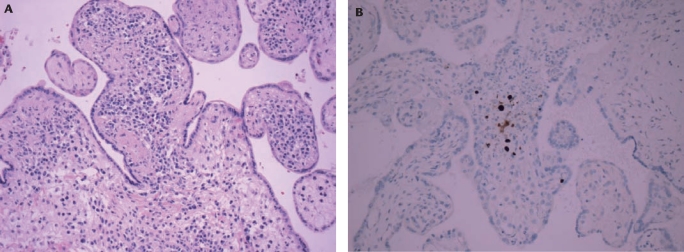
Maternal serologic tests performed in light of the ultrasound findings revealed elevated CMV IgM and IgG titers. Amniotic fluid was strongly positive for CMV DNA by quantitative real-time polymerase chain reaction (RT-qPCR).
After extensive counseling as to the diagnosis of fetal CMV and their options, including pregnancy termination, the couple chose to continue the pregnancy. After consultation with an infectious disease specialist, CMV immune globulin (200 U/kg, for a total dose of 10 g intravenous [IV]) was recommended starting at 25 weeks of gestation with subsequent doses of 5 g IV planned at monthly intervals. Fetal magnetic resonance imaging (MRI) at 25 weeks of gestation showed no evidence of intracranial calcifications or abnormalities.
At 30 weeks, the woman gave birth to a female baby. The neonate was intubated and admitted to neonatal intensive care. Chest radiography showed ground glass opacities consistent with congenital CMV pneumonia. Hematologic abnormalities included thrombocytopenia, coagulopathy, elevated transaminase levels, and hyperbilirubinemia. CMV antigenemia was present in the infant’s blood, and CMV DNA was identified in urine and cerebrospinal fluid.
The infant was treated with IV gancyclovir (6 mg/kg twice daily) with subsequent resolution of laboratory and imaging abnormalities over a 10-day period. Ultrasound examination of the head and abdomen showed no evidence of calcifications, ventriculomegaly, or hepatosplenomegaly prior to treatment. Ophthalmologic examination showed no evidence of retinitis. However, the infant failed multiple newborn hearing screens and appeared to have profound bilateral deafness. Antiviral therapy was continued for 6 weeks. The infant was discharged home in stable condition on day of life 55.
Maternal serologic tests performed in light of the ultrasound findings revealed elevated CMV IgM and IgG titers. Amniotic fluid was strongly positive for CMV DNA by quantitative real-time polymerase chain reaction (RT-qPCR).
After extensive counseling as to the diagnosis of fetal CMV and their options, including pregnancy termination, the couple chose to continue the pregnancy. After consultation with an infectious disease specialist, CMV immune globulin (200 U/kg, for a total dose of 10 g intravenous [IV]) was recommended starting at 25 weeks of gestation with subsequent doses of 5 g IV planned at monthly intervals. Fetal magnetic resonance imaging (MRI) at 25 weeks of gestation showed no evidence of intracranial calcifications or abnormalities.
At 30 weeks, the woman gave birth to a female baby. The neonate was intubated and admitted to neonatal intensive care. Chest radiography showed ground glass opacities consistent with congenital CMV pneumonia. Hematologic abnormalities included thrombocytopenia, coagulopathy, elevated transaminase levels, and hyperbilirubinemia. CMV antigenemia was present in the infant’s blood, and CMV DNA was identified in urine and cerebrospinal fluid.
The infant was treated with IV gancyclovir (6 mg/kg twice daily) with subsequent resolution of laboratory and imaging abnormalities over a 10-day period. Ultrasound examination of the head and abdomen showed no evidence of calcifications, ventriculomegaly, or hepatosplenomegaly prior to treatment. Ophthalmologic examination showed no evidence of retinitis. However, the infant failed multiple newborn hearing screens and appeared to have profound bilateral deafness. Antiviral therapy was continued for 6 weeks. The infant was discharged home in stable condition on day of life 55.

Prevention and Control of CMV:

- A common mode of CMV transmission to a pregnant woman is through close contact with infected bodily fluids such as urine or saliva, especially from young children.
- There is no vaccine and treatment is limited, prevention such as good hand hygiene should be used.
- These practices have been encouraged by organizations such as CDC and the American College of Obstetricians and Gynecologists (ACOG), which recommend that obstetricians and gynecologists (OB/GYNs) counsel women on careful handling of potentially CMV-infected articles, such as diapers, and thorough hand washing after close contact with young children
- Despite this increased emphasis on avoiding infection during pregnancy, few women are aware of CMV infection and how it can be prevented During March--May 2007, ACOG surveyed a national sample of OB/GYNs to assess their knowledge and practices regarding CMV infection prevention, which indicated that fewer than half (44%) of OB/GYNs surveyed reported counseling their patients about preventing CMV infection. Thus, the need for additional training regarding CMV infection prevention is needed for OB/GYNs to have a better understanding during patient counseling.
My Recommendations:
- Due to the fact there is no vaccine I think that the only way to prevent this disease is through patient education.
- Prevention should be focused primarily on mothers of small children, since 80% of young children will develop CMV within 2 years and although they are typically asymptomatic they will continue to shed the virus for years after the intial transmission.
- Hand washing, gloves for diaper changes and avoiding certain types of intimate contact (sharing utensils, kissing on the lips).
- Blood screening and amniocentesis are also necessary in prevention.
Sources:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3046747/
